In today’s data-driven healthcare landscape, the potential for valuable insights is vast, but so is the risk of data overload. Clinicians and coding teams face the challenge of navigating massive amounts of patient data, from lab results and progress notes to specialist reports and diagnostic tests. Hidden within this sea of information are critical details needed to document chronic conditions, meet MEAT criteria, and ensure compliant HCC coding.
Without the right tools, important diagnoses often go undocumented, RAF scores decline, and clinical teams experience burnout. AI-powered HCC coding that uses aggregated and filtered data transforms complex information into clear, actionable insights. By leveraging artificial intelligence, organizations can streamline chart reviews, uncover more conditions, and provide timely support to clinicians at the point of care, all without overwhelming them.
But even with AI-driven solutions, challenges remain, especially when relying on traditional chart review methods. Let’s explore why these approaches often fall short.
Why traditional chart reviews fall short
A clinician’s time is limited, yet traditional workflows often expect them to dig through a patient’s chart, which could be hundreds to thousands of pages, depending on the patient’s history, to catch a missed diagnosis or confirm a suspected condition. The reality? It’s not feasible.
Chart preppers or coding teams may help by pulling key data into summaries, but without intelligent filtering, even these summaries can be bloated and unhelpful. The core challenge is that raw data is not the same as relevant data. Even software that aggregates data from multiple sources often lacks the ability to prioritize what truly matters.
This inefficiency leads to:
-
- Missed or outdated diagnoses
- Unreliable suspect condition lists
- Extra work for clinicians with little added value
- Risk of non-compliance in risk adjustment programs
That’s why the future lies in AI-powered chart review automation, especially when paired with smart data aggregation and clinical data filtering.
Aggregated and filtered data: What it means for HCC coding
Aggregated data means pulling together disparate pieces of a patient’s medical history (from EHRs, claims, lab systems, and third-party reports) into a single, consolidated view. Filtered data means sifting through that aggregation to isolate what’s clinically significant, current, and relevant for coding.
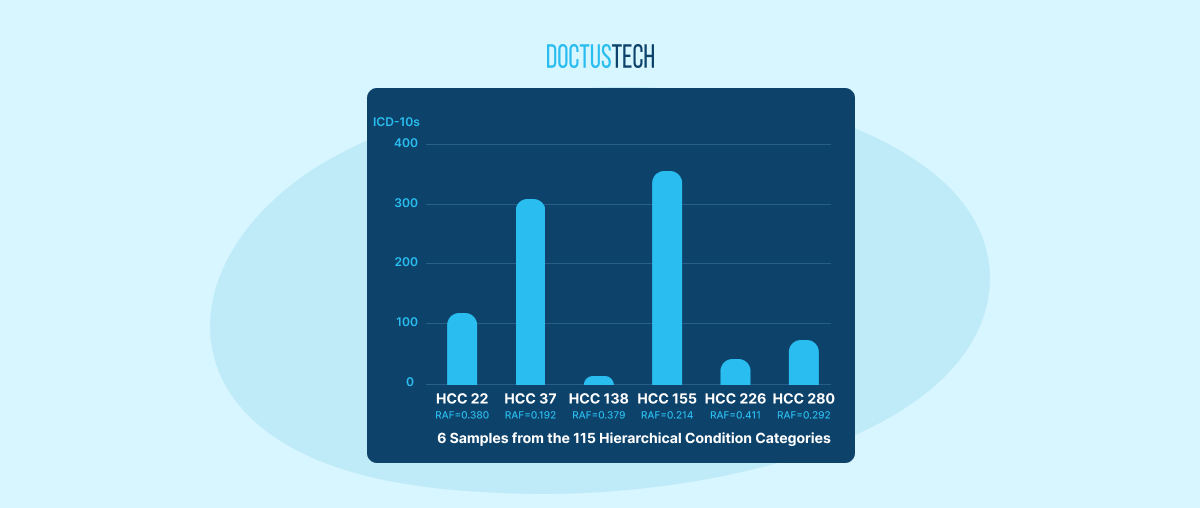
Let’s take an example. A patient has 12 eGFR results in their chart from the past five years:
-
- Only two of them suggest possible chronic kidney disease (CKD).
- The remaining are either outdated or fall within the normal range.
Without intelligent filtering, clinicians or coders may be shown every abnormal lab value, regardless of relevance, forcing them to sift through data to determine clinical significance, making it harder to focus on what truly matters. AI-enhanced filtering improves the process by only surfacing lab patterns consistent with active chronic diseases.
For example, in the case of CKD, the AI looks at the most recent eGFR to check if it is abnormal and if there is another abnormal eGFR from at least three months ago without a normal value in between. This ensures that resolved cases, like someone who had stage 3a CKD two years ago but has since had normal labs, and acute cases, like someone who had a temporary decrease in eGFR, are not mistakenly flagged.
The AI presents this context so the clinician can confidently document CKD when criteria are met or receive guidance to retest when the pattern is unclear.
In the context of HCC coding, this level of intelligent filtering is not just helpful, it’s essential.
How AI transforms chart reviews
AI models trained for HCC coding don’t just pull lab values or diagnoses, they evaluate them in context. They examine trends over time, flag inconsistencies, and even identify when a diagnosis may have been ruled out or resolved. This goes far beyond simple keyword matching or static templates.
Here’s how AI-powered HCC coding with aggregated and filtered data works:
1. Ingests Multiple Data Types
Including structured fields (like ICD-10 codes) and unstructured notes (like free-text progress notes, specialist reports, and radiology impressions).
2. Applies Temporal Logic
It understands whether a condition is active, resolved, or suspected based on its appearance (and disappearance) in the patient timeline.
3. Surfaces Actionable Diagnoses
Instead of flooding the clinician with everything ever recorded, it brings forward only what needs to be reviewed, updated, or confirmed in the current year.
4. Filters Out Irrelevant Noise
Suppresses duplicative or outdated findings (e.g., old claims for ruled-out conditions, resolved injuries) so clinicians aren’t distracted by clutter.
5. Supports Suspecting and Reconciliation
Identifies where diagnoses are likely present but undocumented, and helps close those gaps while ensuring compliance with MEAT documentation standards.
The result? Chart review automation that actually works.
Why claims data alone can’t be trusted
One of the most common sources for suspect condition lists is claims data. While useful, claims often reflect intent rather than confirmed diagnoses. For instance:
-
- A clinician orders an echocardiogram for heart failure based on clinical evaluation.
- The generated claim shows the patient has heart failure.
- The test is negative, and the diagnosis is never made.
If this data is used to generate suspect lists, clinicians are burdened with false positives, chasing diagnoses that were never real. AI helps fix this by interpreting the surrounding data (e.g., test results, subsequent care plans) to determine if a diagnosis is still “in play” or no longer relevant.
Key clinical data types for AI filtering
To drive accurate risk adjustment and compliant coding, the AI model must pull from a wide spectrum of clinical sources. The most impactful include:
-
- Lab Results: Especially for conditions like diabetes (A1C), CKD (eGFR), heart failure (BNP), or rheumatoid arthritis (RF).
-
- Progress Notes: Often the richest source for diagnosis documentation, but hardest to parse manually.
-
- Claims History: Useful, but must be contextualized by AI.
-
- Medication Records: AI can help flag certain prescriptions that can point to possible underlying conditions. For example, insulin may suggest diabetes, antiarrhythmics may indicate atrial fibrillation, and bronchodilators can be a clue for COPD.
-
- Specialist Reports: Help validate complex or chronic diagnoses like cancer, heart failure, or autoimmune diseases.
-
- Imaging and Diagnostics: Can support or refute suspect conditions.
AI can combine these into a cohesive narrative of the patient’s clinical reality, surfacing only what’s current, relevant, and worth documenting.
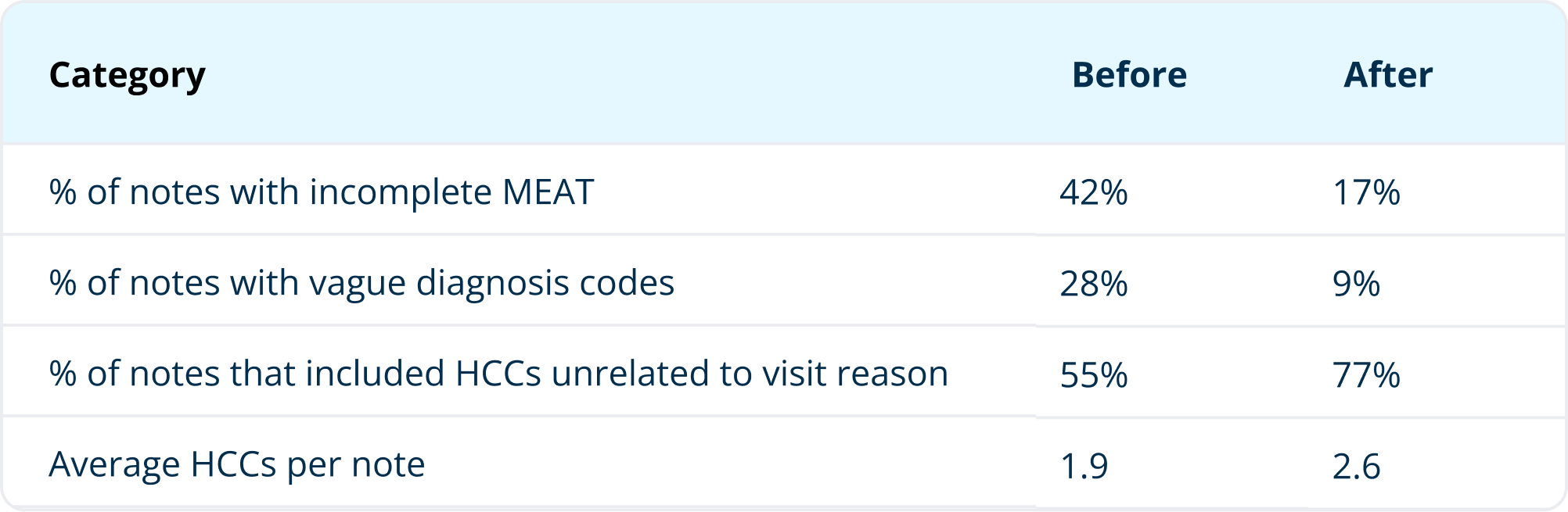
From manual reviews to meaningful action
By applying AI-powered aggregation and filtering, health organizations can drastically reduce the manual work required to support accurate HCC coding.
Let’s compare traditional software with AI-powered workflows:
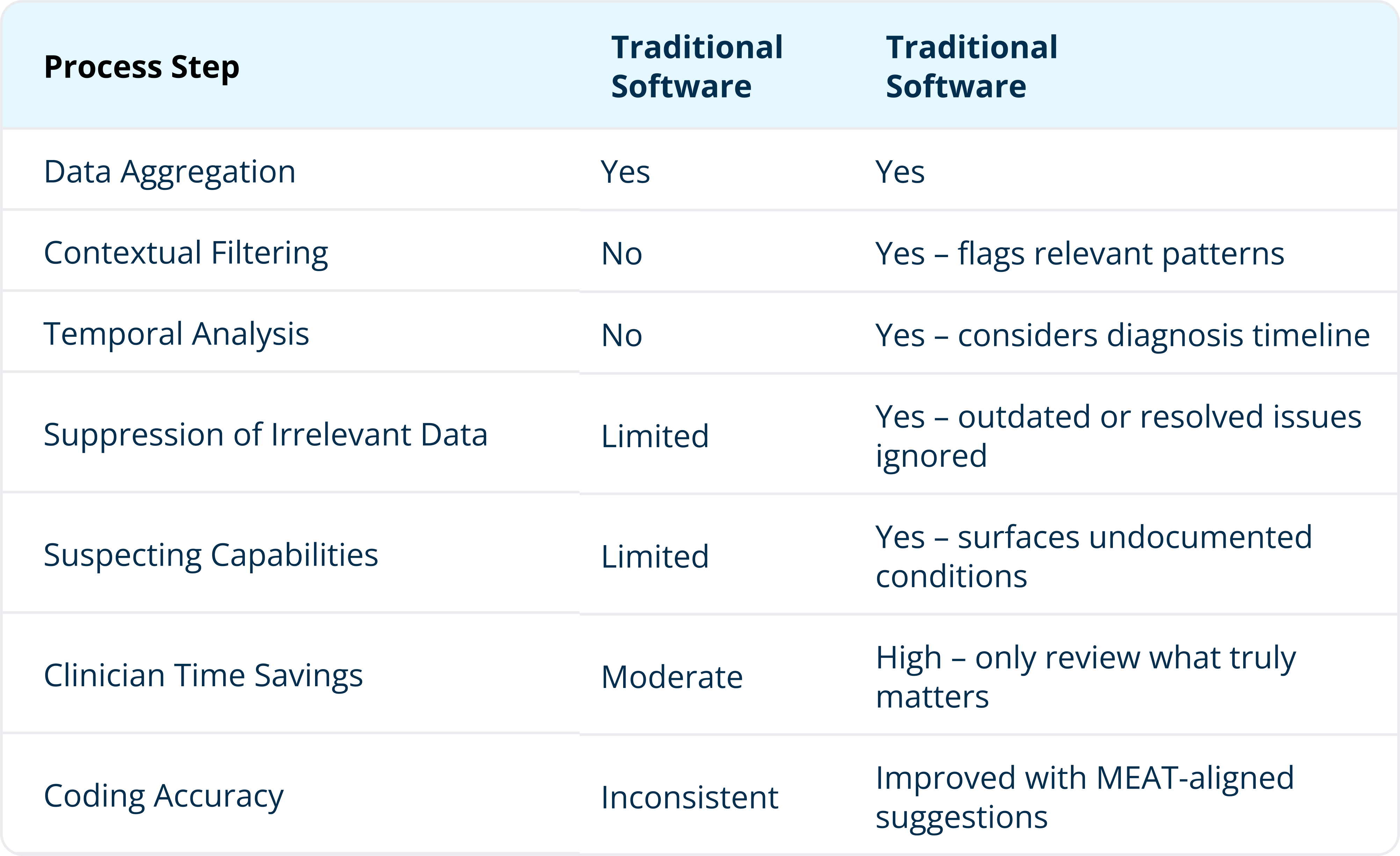
Clinician benefits at the point of care
Ultimately, this approach isn’t just about better coding, it’s about supporting better care delivery. When clinicians are equipped with high-confidence, AI-curated summaries that highlight true coding opportunities, they can:
-
- Make faster, more accurate documentation decisions
- Spend less time on chart review
- Maintain compliance with less stress
- Focus more on clinical judgment, less on paperwork
In a value-based care world, this translates directly into stronger performance on quality and financial metrics.
AI-powered HCC coding is no longer optional
As risk adjustment becomes more complex and clinicians face greater demands on their time, relying on outdated chart review methods is no longer sustainable. The combination of aggregated and filtered data, processed intelligently by AI, represents a turning point in how healthcare organizations approach HCC coding.
This isn’t just about automation. It’s about turning noise into insight, supporting documentation accuracy, and protecting clinical time.
That’s where platforms like DoctusTech come in.
Built specifically for the challenges of HCC coding in value-based care, DoctusTech uses AI to aggregate multi-source data, intelligently filter it for clinical relevance, and present it in a way that actually helps clinicians, not burdens them. The platform identifies undocumented conditions, suppresses irrelevant clutter, and aligns with MEAT documentation standards, all while integrating seamlessly into daily workflows.
With DoctusTech, your team gets:
-
- Actionable summaries, not just raw data
-
- Point-of-care support without workflow disruption
-
- Improved coding accuracy through compliant suggestions
-
- Less burden on clinicians, more focus on patient care
- Less burden on clinicians, more focus on patient care
In a world where every documented diagnosis affects care delivery, compliance, and reimbursement, AI-powered HCC coding with aggregated and filtered data isn’t just a tech upgrade, it’s a strategic advantage.
If your organization is ready to simplify HCC workflows and strengthen risk adjustment performance, DoctusTech is ready to help.
Discover how AI can transform your coding accuracy and support your clinical team, without adding more to their plate. Schedule a demo today.