In an era where efficiency and accuracy in medical documentation are paramount, automated chart reviews with AI are revolutionizing how healthcare professionals handle patient data. Traditional chart reviews, often time-consuming and limited in scope, are now being enhanced with AI-driven tools that streamline the process, reduce human errors, and improve compliance with medical regulations.
This article explores how AI-powered chart reviews work, their benefits over manual reviews, their challenges and misconceptions, and how they can enhance clinician workflows.
The Traditional vs the AI-Powered Approach to Chart Reviews
Historically, chart reviews have relied on manual audits performed by medical professionals. These reviews involve selectively analyzing a small sample of patient records to assess compliance, coding accuracy, and documentation completeness. However, manual reviews present significant limitations:
-
- Limited Scope: Reviewers can only assess a fraction of patient charts due to time constraints.
- Human Error: Even experienced professionals may overlook patterns or misinterpret documentation.
- Time and Resource Intensive: Reviewing large volumes of charts requires significant manpower and time.
With AI-powered chart reviews, technology can analyze entire datasets of patient records in real time. Unlike human auditors who can only evaluate limited samples, AI tools can process vast amounts of medical data instantly, identifying patterns, inconsistencies, and missing documentation with unparalleled accuracy. This is How AI-Powered Chart Reviews Differ from Traditional Methods:
-
- Comprehensive Analysis: AI scans every patient record rather than relying on a small, random sample.
- Error Reduction: AI models detect inconsistencies and missing documentation with greater precision.
- Efficiency: Automating reviews allows for continuous monitoring, ensuring compliance with evolving medical regulations.
- Pattern Recognition: AI can identify trends in documentation, such as common coding errors or missing clinical indicators.
AI vs. Standard Software Tools in Chart Reviews
While traditional software programs can assist with documentation, they typically function using rule-based searches, limiting their flexibility. Unlike traditional rule-based programs, Chart Reviews with AI can interpret context and adapt to different documentation styles, making it a more effective tool for identifying compliance gaps.
For instance, a basic software program may simply flag whether a condition is mentioned in a patient’s chart, whereas AI can assess whether the condition is sufficiently documented based on clinical guidelines. This contextual awareness makes AI superior to simple searches, reducing false positives and improving accuracy.
One of the biggest challenges with standard software tools is their reliance on keyword searches. A simple program might flag every mention of “heart failure” in a patient’s records, but it won’t distinguish between “ruled out heart failure” and an actual diagnosis. AI, however, is being trained to understand nuanced medical language, including whether a clinician is documenting a confirmed condition, considering it as a possibility, or ruling it out entirely. Unlike traditional systems that operate with rigid, rule-based searches, AI has the potential to evaluate whether a condition is documented in compliance with MEAT (Monitor, Evaluate, Assess, and Treat) criteria.
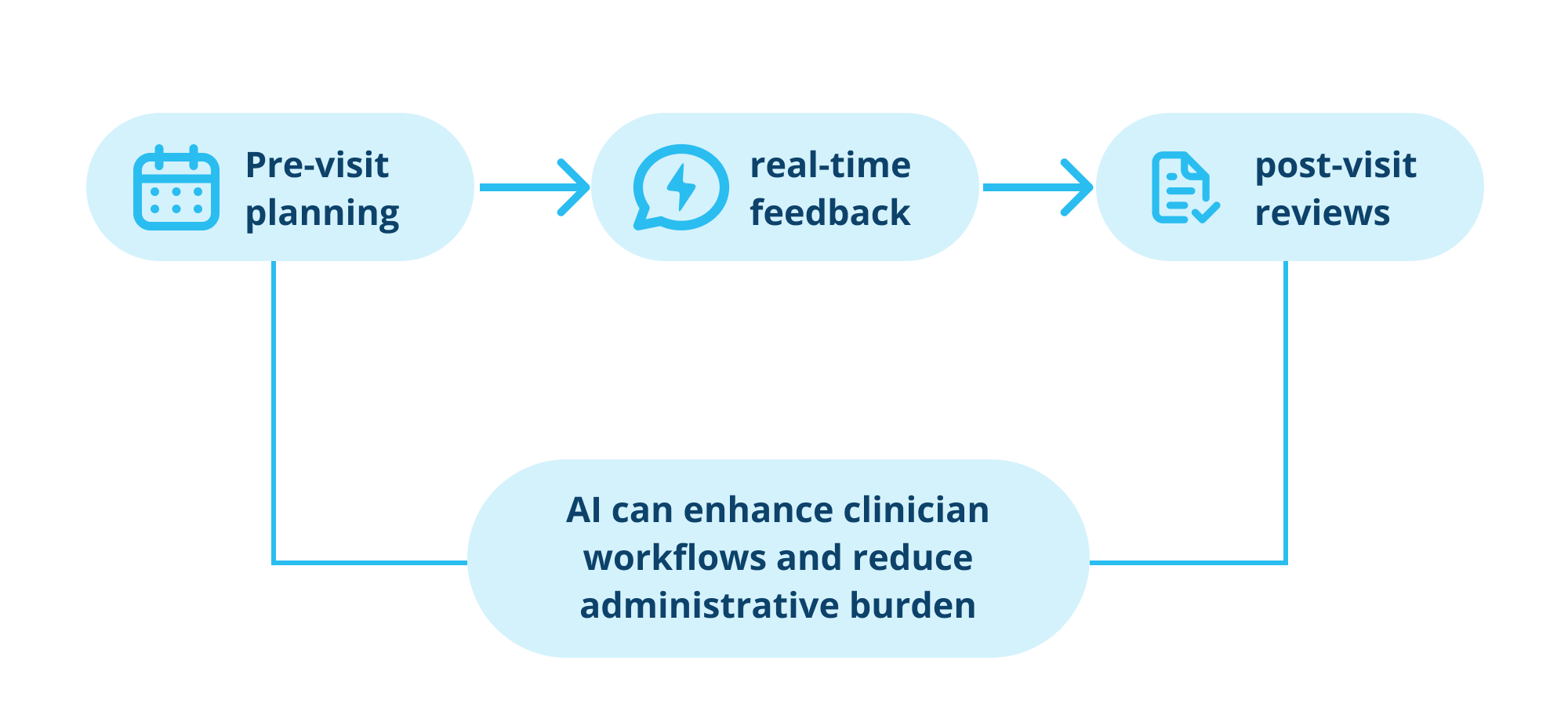
Beyond improving accuracy, AI-driven tools also enhance clinician efficiency by integrating seamlessly into existing workflows:
-
- Pre-Visit Planning: AI highlights relevant patient history, chronic conditions, and potential compliance risks before a consultation, helping clinicians prepare more effectively.
-
- Real-Time Feedback: Clinicians receive instant alerts if documentation is incomplete or non-compliant, reducing the risk of audit penalties.
-
- Post-Visit Reviews: AI reviews recent consultations to ensure coding accuracy and compliance with regulatory requirements, helping maintain accurate and complete documentation.
-
- Reducing Administrative Burden: By automating documentation checks, AI allows clinicians to spend less time on paperwork and more time on patient care.
Despite these advantages, AI still requires refinement. Clinicians document information in varying ways, which can confuse AI models. For example, determining whether a condition is being actively monitored or simply mentioned can be challenging due to differences in writing styles, abbreviations, and phrasing. AI-powered tools must continuously learn from edge cases to improve their accuracy, reducing false positives and negatives.
Addressing Compliance and Regulatory Concerns
Chart Reviews with AI play a critical role in ensuring compliance with regulations such as CMS (Centers for Medicare & Medicaid Services) guidelines. By analyzing medical records against predefined compliance criteria, AI can detect documentation gaps before they become audit issues. This proactive approach minimizes the risk of penalties and ensures that healthcare providers maintain accurate patient records.
However, AI is not yet capable of fully replacing human coders. Regulations and coding guidelines frequently change, requiring ongoing updates to AI models. While AI can flag documentation errors and suggest corrections, human oversight remains essential for addressing complex cases and interpreting nuanced medical data.
However, AI is not a perfect solution, and its role is often misunderstood. Despite the promise of AI in chart reviews, there are several misconceptions that need to be addressed:
1.AI Will Replace Human Coders: While AI significantly reduces the workload of medical coders, human oversight is still required for complex cases and regulatory updates.
2.AI is 100% Accurate: AI-driven tools require continuous refinement to improve accuracy and minimize false positives.
3.AI Works Without Human Input: AI systems rely on predefined parameters and training data, meaning they still need human supervision and continuous learning.
Beyond these misconceptions, AI adoption in medical coding faces real challenges.
Challenges and Limitations of Chart Reviews with AI
Although Chart Reviews with AI have the potential to greatly enhance accuracy and efficiency, it depends on large volumes of high-quality data. However, healthcare documentation can vary significantly across clinicians, specialties, and institutions, which presents several challenges when AI analyzes medical records. Here are some of the common challenges AI faces in interpreting medical documentation:
-
- Understanding Variability in Clinical Documentation: Clinicians document diagnoses differently, making it difficult for AI to interpret all variations accurately. Unlike traditional software that simply checks for documentation presence, AI must determine whether a condition meets compliance criteria, such as the MEAT framework. This involves distinguishing between phrases like “monitoring heart failure” and “heart failure considered and ruled out.”
-
- False Positives and False Negatives: Because clinical language is often inconsistent, AI may flag conditions incorrectly. For example, if a clinician writes “patient screened for diabetes, results negative,” a keyword-based system might incorrectly categorize this as a documented diagnosis. AI models must continuously refine their understanding to avoid such misinterpretations.
-
- Complex Sentence Structures: Clinicians often phrase evaluative statements in unique ways, making it difficult for AI to determine whether a condition is worsening, stable, or improving. Unlike humans, AI struggles with ambiguous language and varying documentation styles, requiring ongoing training to handle edge cases.
-
- User Adoption: Clinicians may be hesitant to rely on AI-driven tools, especially if they are not well integrated into existing workflows. If AI frequently misflags conditions or requires excessive manual corrections, trust in the technology diminishes.
-
- Changing Regulatory Standards: AI systems must be continuously updated to align with evolving medical coding regulations. A model that works well today may need adjustments tomorrow as guidelines shift.
By tackling common misconceptions and challenges, healthcare organizations can unlock the full potential of AI-driven chart reviews—improving accuracy, efficiency, and compliance—without over-relying on the technology or overlooking the value of human oversight.
As the technology evolves, AI’s ability to process vast amounts of medical data far exceeds traditional methods, and chart reviews will only become more effective at reducing administrative burden and supporting regulatory adherence.
Real-World AI Integration: DoctusTech’s PDAP
One example of AI transforming automated chart reviews is DoctusTech’s Patient Diagnosis Assist Platform (PDAP). This AI-driven tool integrates with over 70 major EMRs, allowing clinicians to streamline the redocumentation process without switching between portals or dealing with paper-based systems.
DoctusTech enhances pre-chart planning with:
-
- Automated Chart Reviews: AI translates patient charts into accurate HCC codes in seconds, saving up to 2.5 hours per week per clinician on documentation.
-
- Faster Progress Notes: By aggregating all relevant data directly into the EMR, clinicians can complete notes efficiently with 100% satisfaction.
-
- Huddle Board: A feature that streamlines patient encounter management, displaying visit types, screening tests, and action items for optimized workflows.
Final Thoughts: Chart Reviews with AI for Smarter Healthcare
Chart Reviews with AI represent a transformative shift in healthcare documentation, improving accuracy, compliance, and efficiency. AI enables healthcare providers to focus on delivering high-quality patient care by improving accuracy, enhancing compliance, and reducing administrative burdens.
While challenges remain, ongoing advancements in AI technology and seamless integration into clinical workflows will ensure that AI becomes an indispensable tool in medical chart reviews. The future of healthcare documentation is here, and AI is leading the way.
Ready to see how DoctusTech can help? Schedule a demo today and discover how DoctusTech can transform your pre-charting and HCC coding processes.