
WHAT IS CHANGING IN HCC V28?
Widespread changes to the CMS risk adjustment model are coming in 2024. Although the final details, the anticipated impact of the changes, and what it will mean for risk adjustment are yet to be seen, we wanted to give you some insight into the details of these proposed changes.
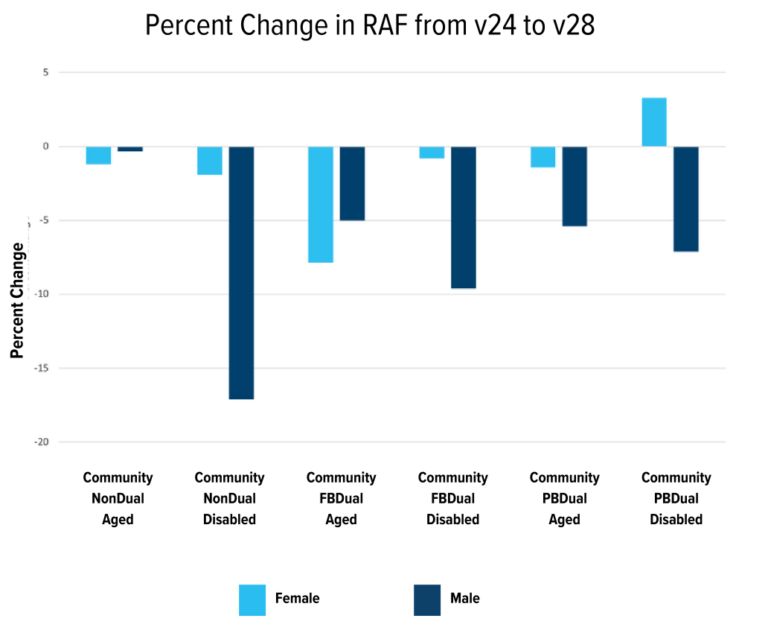
CHANGES IN DEMOGRAPHIC CALCULATIONS
We will begin by looking at demographic rates. Each patient in the HCC model is given a base risk adjustment number based on: 1) their sex, 2) disability status, and 3) full or partial dual eligibility (for Medicare/Medicaid). The changes in demographic rates from v24 to v28 are expected to drop on average across all categories by -1.65% in females and -7.43% in males. Most groups had a 1% to 5% decrease, but it is worth noting that the most significant changes were all seen in disabled populations. The community, non-dual-eligible males had a 7.11% decrease across all ages, the fully dual-eligible males had a -9.60% change, and the partially dual-eligible males had a -7.11% change. Interestingly, the only grouping whose average score increased was the partially dual-eligible females, with a 3.29% average increase.
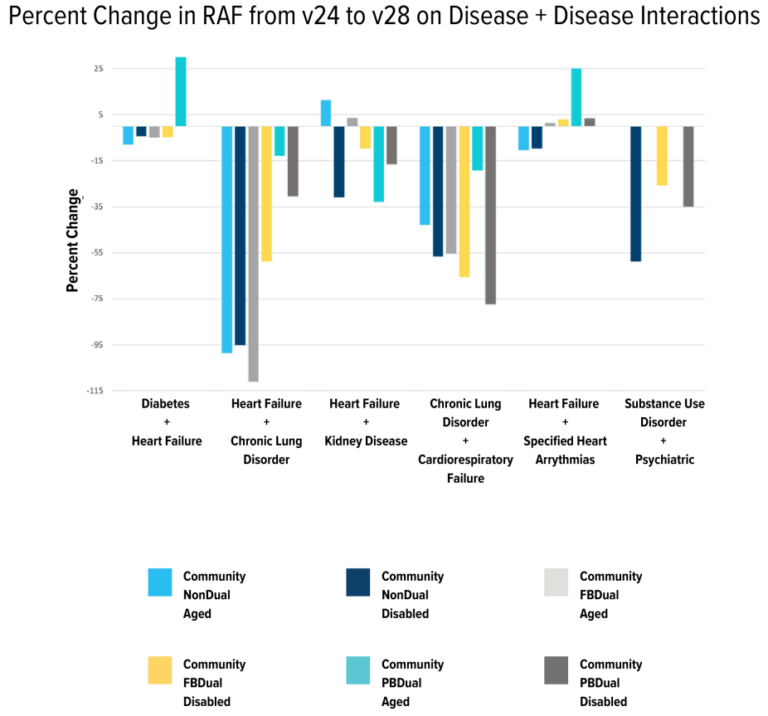
Disease + disease interaction modifiers is another variable impacted by v28. (For example, if a patient is coded with both diabetes and CHF, an additional modifier is added to the score). Although HCCs were rearranged into new categories, all of the interaction categories from v24 are still present in v28, with one exception: immune disorders + cancer. The interaction of immune disorders and cancer traditionally added an additional RAF of 0.6-0.8 to each patient.
Looking at the values of the interaction categories, the value of most groups decreased by 12% – 70%. Notably, two particular groupings had substantial increases and deviated from the other trends. These are the interaction of CHF and diabetes and the interaction between CHF and arrhythmias, both in partially dual-eligible aged populations, with an increase of 31% and 25%, respectively.
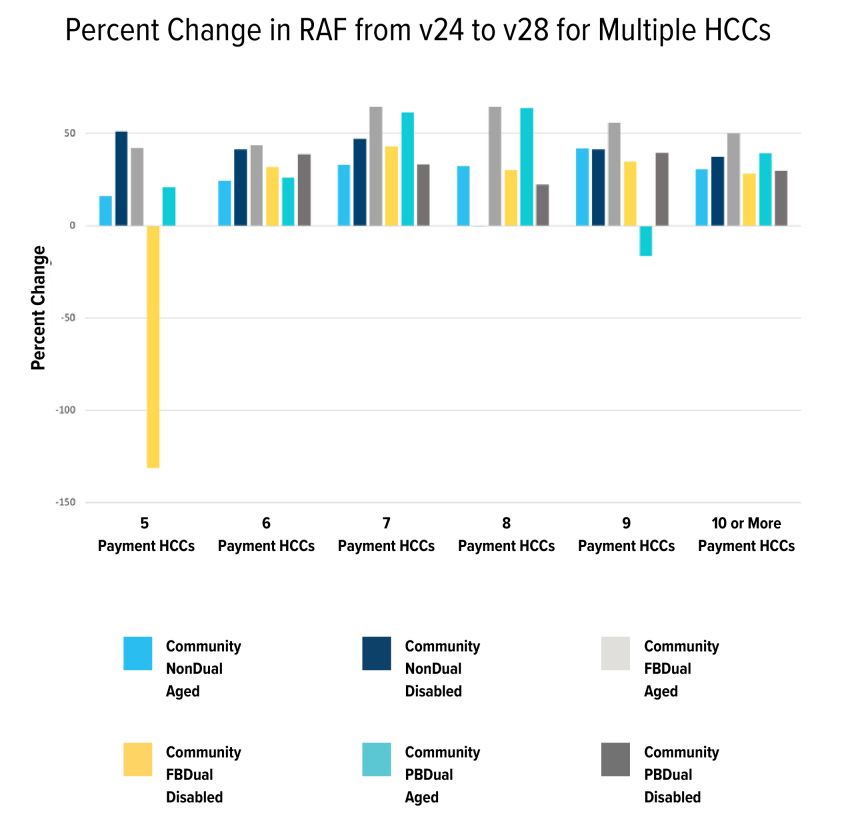
The last add-on metric to look at is the additional value that is added for having a large number of different HCC categories. Patients with five or more different HCCs will have an additional value added as each added diagnosis increases complexity, with the add-on capping out at ten different HCCs. Unlike the previous categories, the changes from v24 to v28 result in a higher value being added to the patient’s risk score in almost every possible grouping. On average, these scores have increased by 37.06%.
RAW RAF ADJUSTERS
After a patient’s total RAF is calculated, it undergoes two further calculations. First is the normalization ratio calculation. CMS creates this number by looking at the average cost of care and health status of fee-for-service patients over a 5-year period. Once an average RAF is determined from this data, they calculate what number needs to be multiplied by that value to equal 1.0. This number is the ‘normalization ratio.’ The ratio is then divided by the patient’s raw RAF score to ‘normalize’ the average health status of a patient. Previously, this number was 1.127, meaning a patient with a total RAF of 3.2 would only be counted as if they had 2.84. The v28 2024 proposed normalization ratio is 1.015. Using the new ratio, the same total RAF of 3.2 will be calculated as 3.15. This means that every patient’s final RAF will be around 10% higher.
The last calculation that is performed takes place after normalization. This calculation is referred to as the “MA coding adjustment.” This is a percent decrease in RAF that is added to compensate for the difference in coding practices between risk adjustment coders and fee-for-service coders. This percentage has maintained at 5.9% for some time and is not proposed to change in v28.
HCC NUMBERINGS
The v24 model of managed care used ICD-9 codes as its basis for HCC categorization. CMS has now transitioned to ICD-10 as its reference, allowing for more specificity in charting and grouping. In v28, the total number of HCCs increases from 86 to 115, while the number of codes that map to an HCC diagnosis decreases from 9,797 to 7,770. CMS separates the 115 HCCs into 26 groupings of conditions, and conditional hierarchies are also contained in these groupings.
The main call-outs on deletions include:
- Removal of secondary hypercoagulable state
- Removal of stable angina
- Removal of an immunocompromised state
- Removal of almost all forms of PVD
- Removal of ‘other endocrine abnormalities’ such as secondary hyperparathyroidism and secondary hyperaldosteronism.
- Removal of protein-calorie malnutrition
IN CONCLUSION
It is no secret that a wide variation of HCC coding patterns exist among clinical groups engaged in the Medicare Advantage program. v28 will eliminate many of the diagnoses that are found through careful screening or loosely defined clinical judgment.
Regardless of where you sit philosophically on the debate, the following will undoubtedly occur:
- Increased importance of clinician training as their decision-making will outperform other current strategies for HCC optimization.
- Regression of patient RAF towards the mean, specifically for those in the top percentile.
- Reduced impact of annual wellness visits for coding optimization.
- Reduced impact of retrospective chart reviews and third-party annual wellness visit companies for engaged patients. (Most of these codes will have already been picked up by their PCPs, no more esoteric diagnoses.)
CONTACT YOUR CUSTOMER SUCCESS ASSOCIATE IF YOU WOULD LIKE:
- To have a one-time audit done on your current claims data to estimate the impact on RAF
- Help to streamline documentation accuracy within your EMR with DoctusTech’s integrated solution